Processing Your Payment
Please do not leave this page until complete. This can take a few moments.
-
News
-
Editions
-
- Lists
-
Viewpoints
-
HBJ Events
-
Event Info
- 2024 Economic Outlook Webinar Presented by: NBT Bank
- Best Places to Work in Connecticut 2024
- Top 25 Women In Business Awards 2024
- Connecticut's Family Business Awards 2024
- What's Your Story? A Small Business Giveaway 2024 Presented By: Torrington Savings Bank
- 40 Under Forty Awards 2024
- C-Suite and Lifetime Achievement Awards 2024
- Connecticut's Health Care Heroes Awards 2024
-
-
Business Calendar
-
Custom Content
- News
-
Editions
View Digital Editions
Biweekly Issues
- April 29, 2024
- April 15, 2024
- April 1, 2024
- March 18, 2024
- March 4, 2024
- February 19, 2024
- February 5, 2024
- January 22, 2024
- January 8, 2024
- + More
Special Editions
- Lists
- Viewpoints
-
HBJ Events
Event Info
- View all Events
- 2024 Economic Outlook Webinar Presented by: NBT Bank
- Best Places to Work in Connecticut 2024
- Top 25 Women In Business Awards 2024
- Connecticut's Family Business Awards 2024
- What's Your Story? A Small Business Giveaway 2024 Presented By: Torrington Savings Bank
- 40 Under Forty Awards 2024
- C-Suite and Lifetime Achievement Awards 2024
- Connecticut's Health Care Heroes Awards 2024
Award Honorees
- Business Calendar
- Custom Content
COVID map turns red: 80% of CT residents in hot zones
 Eighty percent of Connecticut residents now live in COVID hot zones, places where the per-capita caseload exceeds 15 per 100,000 people.
Eighty percent of Connecticut residents now live in COVID hot zones, places where the per-capita caseload exceeds 15 per 100,000 people.
The autumn surge of COVID-19 cases has reached red-alert status in 100 of Connecticut’s 169 cities and towns, with the state’s largest city, Bridgeport, now experiencing the worst outbreak — and with hospitalizations for the disease statewide more than doubling in the past two weeks.
A subdued Gov. Ned Lamont outlined the latest metrics Thursday in the second of his twice-a-week televised briefings, joined by a medical adviser, Dr. Scott Gottlieb, who warned that all epidemiological models indicate cases will continue to increase into the new year.
“I think this is the final stage of the acute phase of this pandemic that we need to get through,” said Gottlieb, the former head of the Food and Drug Administration. “Unfortunately, it’s going to be the hardest phase right now. We’re in for a very difficult two to three months.”
Eighty percent of Connecticut’s population lives in red-alert communities, defined as places where the measure of 15 cases per 100,000 people is exceeded. The rate Thursday was 53.2 cases per 100,000 people in Bridgeport, 49.9 in Danbury, 46.3 in Waterbury, 45.3 in New London and 41.3 in Hartford.
The rolling seven-day average of positive results in COVID-19 tests in the state was 4.4%, but another 33 people were hospitalized for COVID, increasing the daily census to 617 — up from 270 two weeks ago, but far below the peak of 2,000 during the first surge of cases.
“That’s a number I’m watching carefully,” Lamont said.
COVID-19 fatalities rose by 10 in the state, reaching 4,726 since March. Nationally, the death toll has topped 240,000.
Fourteen states reported record COVID-19 hospitalizations Thursday, with the seven-day average of new cases reaching highs in 23 states, according to data tracked by the Washington Post.
Lamont and Gottlieb said they were was less concerned about hospital capacity in Connecticut than the availability of sufficient medical personnel. In the spring and summer, medical personnel were able to go to hotspots like New York City.
“Last time around, we could bring in nurses and specialists from elsewhere,” Lamont said. “There is no elsewhere right now.”
“Now, what we’re seeing is a truly national epidemic where every part of the country is going to be simultaneously engulfed in infection,” Gottlieb said.
Connecticut is better positioned to withstand the latest surge than during the original spread of the novel coronavirus in March, when therapies were limited, the in-hospital mortality rate high and the health care system approached capacity, Lamont and Gottlieb said.
Gottlieb said in-hospital mortality rates have dropped as doctors have used months of experience with novel coronavirus to change treatment regimens, primarily by the aggressive use of steroids, supplemental oxygen and remdesivir, an anti-viral that does not cure COVID-19 but can lessen its impact by hampering the replication of the virus in the body.
Lamont tightened COVID-19 restrictions a week ago, limiting the hours and capacity of restaurants and other public venues. The state now has 200 COVID-19 testing locations, but delays have been reported, primarily due to periodical shortages of collection material, not laboratory backlogs.
The state now is able to trace 98% of people exposed to COVID-19 within 48 hours and reach 65% of them.
Gottlieb said the disease might finally be tamed in 2021. At the current rate of spread, at least 30% of the U.S. will have had the disease, slowing transmission. And mass vaccinations might be available next summer.
He also said the public is growing more educated and cautious about the disease.
“As much as people are getting exhausted, they’re also getting smarter,” Gottlieb said.
A reporter challenged that assertion, noting that there is an anti-mask movement and that the White House has been a COVID-19 hotspot. President Donald J. Trump has ridiculed the wearing of masks, and the president and 14 people in the president’s circle have tested positive.
Gottlieb, a former member of Trump administration, smiled.
“Well,” he said, “some people are getting smarter.”





Here are clinical trials in which remdesivir failed to shorten hospital stays or reduce deaths:
https://www.medrxiv.org/content/10.1101/2020.10.15.20209817v1
https://pubmed.ncbi.nlm.nih.gov/33264556/
https://www.nejm.org/na101/home/literatum/publisher/mms/journals/conten…
https://www.nejm.org/na101/home/literatum/publisher/mms/journals/conten…
https://rebelem.com/remdesivir-in-moderate-covid-19/
https://www.medrxiv.org/content/10.1101/2020.08.10.20171637v1
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7190303/
https://finance.yahoo.com/chart/GILD
{kind=link}
{kind=link}
Remdesivir is totally useless against all viral diseases, including the flu, common cold, and Ebola:
https://www.nejm.org/doi/full/10.1056/NEJMoa1910993
https://www.nejm.org/na101/home/literatum/publisher/mms/journals/conten…
{kind=link}
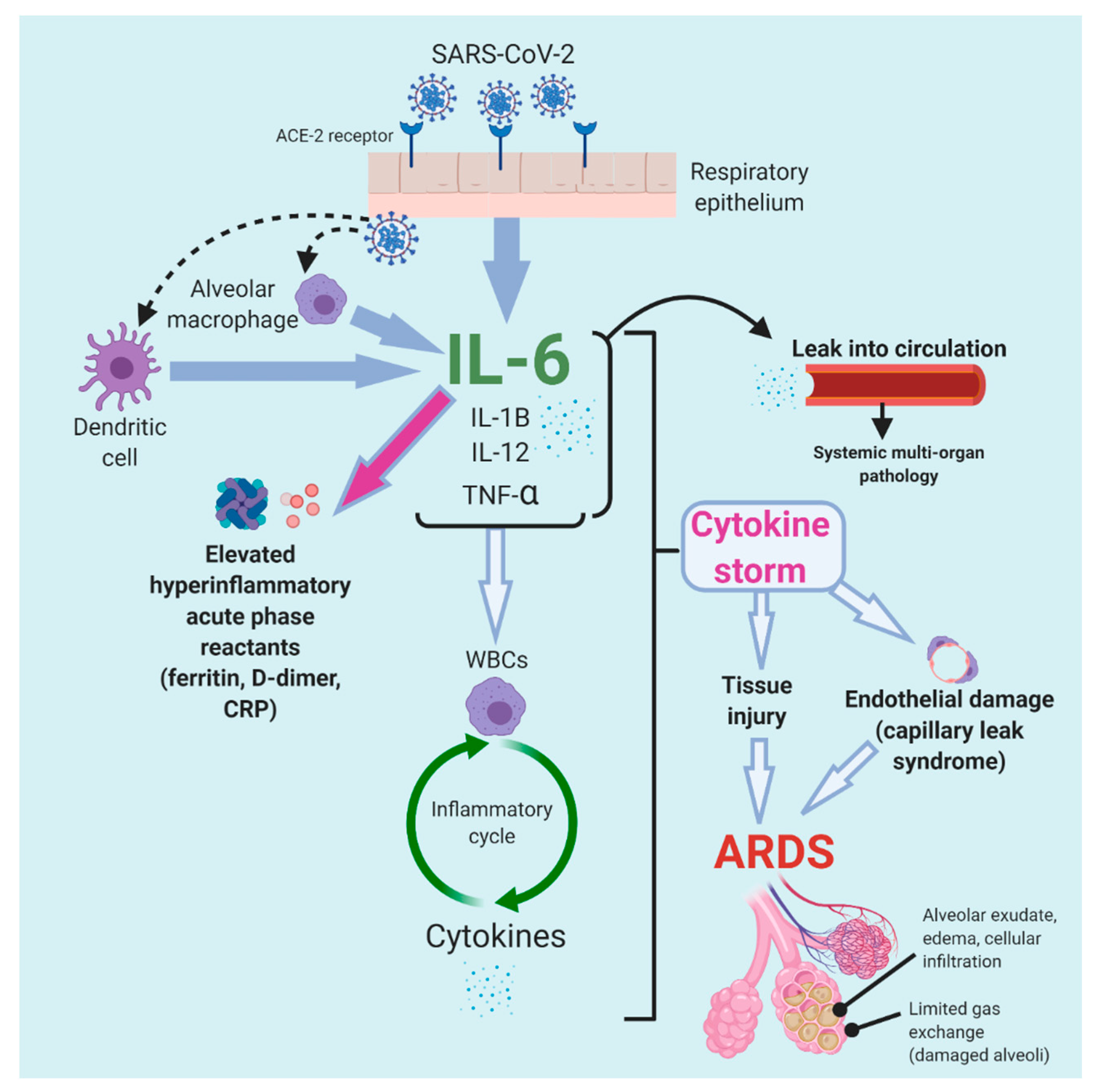
Remdesivir is fraudulently indicated for end-stage COVID-19 when in truth, it has absolutely no benefit in reducing the cytokine storm, in fact, might make it slightly worse:
https://www.nature.com/articles/s41591-020-1051-9
https://www.nature.com/articles/s41591-020-1051-9/figures/5
https://www.mdpi.com/tropicalmed/tropicalmed-05-00112/article_deploy/ht…
{kind=link}
Remdesivir, hydroxychloroquine, and chloroquine cause cardiovascular QT interval prolongation and sinus bradycardia:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7571425/
https://www.sciencedirect.com/science/article/abs/pii/S0022073620305835
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7598346/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7682945/
Remdesivir causes liver damage:
https://theprint.in/health/govt-reviewing-remdesivir-use-for-covid-afte…
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7381904/
https://pubmed.ncbi.nlm.nih.gov/33006138/
Remdesivir causes kidney damage:
https://www.rxlist.com/consumer_remdesivir_rdv/drugs-condition.htm
https://pubmed.ncbi.nlm.nih.gov/33252992/
Here are clinical trials in which remdesivir failed to shorten hospital stays or reduce deaths:
https://www.medrxiv.org/content/10.1101/2020.10.15.20209817v1
https://pubmed.ncbi.nlm.nih.gov/33264556/
https://www.nejm.org/na101/home/literatum/publisher/mms/journals/conten…
https://www.nejm.org/na101/home/literatum/publisher/mms/journals/conten…
https://rebelem.com/remdesivir-in-moderate-covid-19/
https://www.medrxiv.org/content/10.1101/2020.08.10.20171637v1
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7190303/
https://finance.yahoo.com/chart/GILD
Remdesivir is totally useless against all viral diseases, including the flu, common cold, and Ebola:
https://www.nejm.org/doi/full/10.1056/NEJMoa1910993
https://www.nejm.org/na101/home/literatum/publisher/mms/journals/conten…
Remdesivir is fraudulently indicated for end-stage COVID-19 when in truth, it has absolutely no benefit in reducing the cytokine storm, in fact, might make it slightly worse:
https://www.nature.com/articles/s41591-020-1051-9
https://www.nature.com/articles/s41591-020-1051-9/figures/5
https://www.mdpi.com/tropicalmed/tropicalmed-05-00112/article_deploy/ht…
Remdesivir, hydroxychloroquine, and chloroquine cause cardiovascular QT interval prolongation and sinus bradycardia:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7571425/
https://www.sciencedirect.com/science/article/abs/pii/S0022073620305835
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7598346/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7682945/
Remdesivir causes liver damage:
https://theprint.in/health/govt-reviewing-remdesivir-use-for-covid-afte…
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7381904/
https://pubmed.ncbi.nlm.nih.gov/33006138/
Remdesivir causes kidney damage:
https://www.rxlist.com/consumer_remdesivir_rdv/drugs-condition.htm
https://pubmed.ncbi.nlm.nih.gov/33252992/

2022 Giving Guide
This special edition informs and connects businesses with nonprofit organizations that are aligned with what they care about. Each nonprofit profile provides a crisp snapshot of the organization’s mission, goals, area of service, giving and volunteer opportunities and board leadership.
Learn more
Subscribe
Hartford Business Journal provides the top coverage of news, trends, data, politics and personalities of the area’s business community. Get the news and information you need from the award-winning writers at HBJ. Don’t miss out - subscribe today.
Subscribe
2024 Book of Lists
Delivering Vital Marketplace Content and Context to Senior Decision Makers Throughout Greater Hartford and the State ... All Year Long!
Read Here-
2022 Giving Guide
This special edition informs and connects businesses with nonprofit organizations that are aligned with what they care about. Each nonprofit profile provides a crisp snapshot of the organization’s mission, goals, area of service, giving and volunteer opportunities and board leadership.
-
Subscribe
Hartford Business Journal provides the top coverage of news, trends, data, politics and personalities of the area’s business community. Get the news and information you need from the award-winning writers at HBJ. Don’t miss out - subscribe today.
-
2024 Book of Lists
Delivering Vital Marketplace Content and Context to Senior Decision Makers Throughout Greater Hartford and the State ... All Year Long!
ABOUT
ADVERTISE
NEW ENGLAND BUSINESS MEDIA SITES
No articles left
Get access now
In order to use this feature, we need some information from you. You can also login or register for a free account.
By clicking submit you are agreeing to our cookie usage and Privacy Policy
Already have an account? Login
Already have an account? Login
Want to create an account? Register
Get access now
In order to use this feature, we need some information from you. You can also login or register for a free account.
By clicking submit you are agreeing to our cookie usage and Privacy Policy
Already have an account? Login
Already have an account? Login
Want to create an account? Register
2 Comments